LUMBAR FUSION, or ARTHRODESIS, is a procedure that involves immobilising a segment of the spine to prevent the pain caused by the disc and facet joints, to slow the process of disc degeneration, and it is sometimes also used to stabilise the segment after nerve or spinal canal decompression surgery when extensive bone resection is required.
To perform this surgery, special spinal screws connected by rods are used, and a cage-shaped implant is placed between the vertebrae to restore disc height. This system blocks movement and prevents compression of the spinal nerves.
When that segment becomes immobile, spinal biomechanics change; the remaining segments share the load and take on more mobility, which directly and indirectly may cause a previously existing degenerative process to continue or accelerate. Degeneration of the disc adjacent to a lumbar arthrodesis is called “adjacent disc disease”. Although studies report very variable figures, the incidence could be estimated at 16.5% at 5 years and 36.1% at 10 years, i.e., 3 out of 10 operated patients.
In other words, it is clear that the discs adjacent to the fused segment will be more overloaded, but will they fail yes or no? No Not always.
If the degenerative process has already begun in the adjacent disc, we can state that there is a higher likelihood of problems in a few years, but there are more factors that influence this:
- Pre-existing factors, or patient characteristics prior to surgery
- Obesity, due to the chronic weight overload it places on the discs
- When arthrodesis is performed at an older age, the spine has less potential to adapt to the fusion due to greater stiffness, which is associated with a higher likelihood of adjacent disc disease.
- Degenerative disc changes or facet joint alterations already present (just as the operated disc has degenerated, there may be other discs in which the degenerative process has begun).
To address these factors, we always recommend a combined programme of weight loss and muscle training before and after the surgeries we perform. The patient is informed about the condition of their other discs and the likelihood of adjacent disc disease.
- Factors related to the surgical technique:
- Resection of posterior elements in extensive decompressive surgeries.
- Using fusion techniques that do not maintain or restore lumbar lordosis, or not taking the alignment of the rest of the spine into account when planning surgery.
- Performing very rigid fusions
- Extending instrumentation to the sacrum to achieve greater fixation in surgeries where only the posterior elements are fused.
- Fusions of more than two levels: the more discs operated on, the greater the likelihood of overloading adjacent ones.
In this regard, minimally invasive fusion techniques preserve the posterior elements, protecting against adjacent disc disease. We tend to perform fusions at the fewest levels possible, assessing in each case the spinal curves and degenerative changes in adjacent discs. Anterior-approach techniques allow us to better preserve lordosis and respect the facet joints better than any other technique.
When a patient has already undergone spine surgery, we request several tests to study their case. MRI informs us about compression of the spinal canal or of the nerve roots at the foramina; CT is used to check bony fusion and the condition of the screws, whether they are loosened or not; flexion-extension X-rays help detect hidden instability; and a full-spine X-ray is used to assess overall posture and the state of lordosis.
Non-surgical treatment includes weight loss, muscle training, and postural correction. Other alternatives we offer when standard analgesia does not improve symptoms include injections to reduce inflammation in areas of overload:
- facet joint block or radiofrequency
- foraminal injection for sciatica
- caudal epidural block when there is spinal canal stenosis
If conservative treatment does not resolve the problem, the case is already very advanced, or the patient’s function is significantly affected, surgery may be indicated. Each case is unique and requires a personalised assessment.
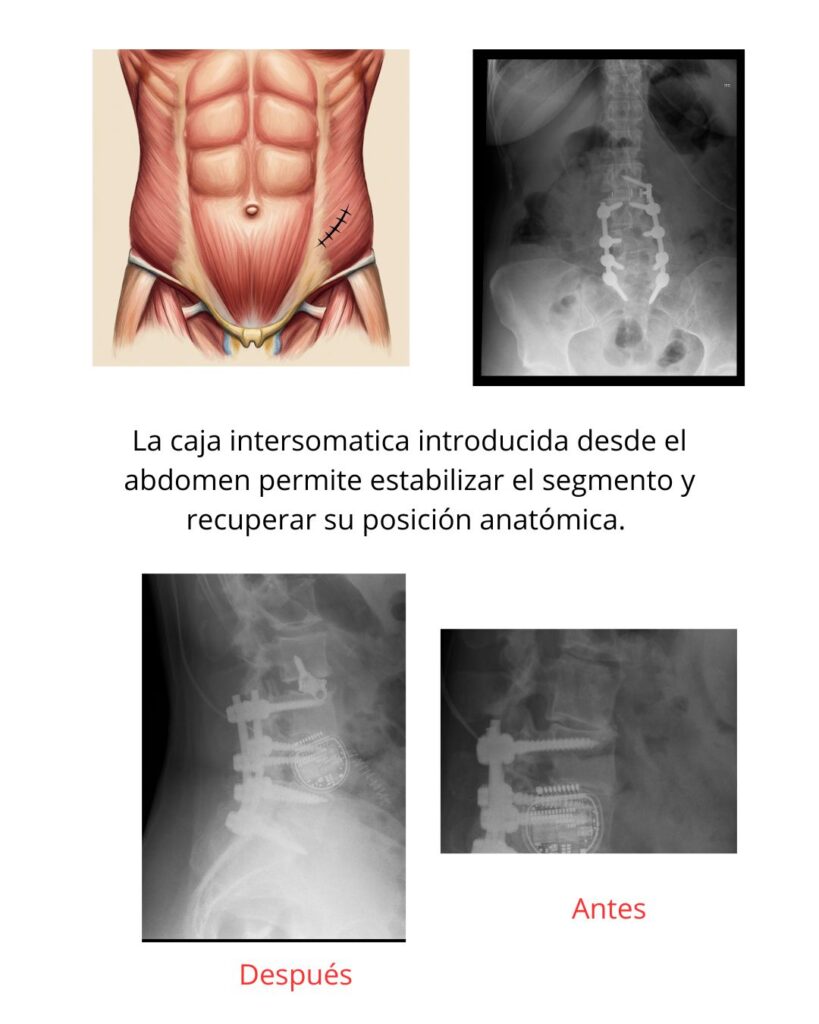
I will show you a case we have resolved via an anterior approach with a very good outcome. I usually prefer the OLIF approach when the patient needs lordosis correction and we do not want to reopen the previous scar to avoid infection-related problems.